
Providing top-notch dental care requires investment in expert staff, high-quality supplies, state-of-the-art equipment, and legally compliant recordkeeping, but these things don’t come cheaply. And, as if that weren’t enough, contracted reimbursement rates from insurance providers and payments from patients often fail to keep pace with rising costs. Two practices might see the same number of patients, but runaway overhead costs can be the difference between one of them struggling to pay the bills and the other generating enough profit to reinvest in upgrading equipment and techniques.
This article breaks down dental office overhead and looks at what it includes, how to calculate it, where the benchmarks fall, and how to cut costs without sacrificing care.
What Is Dental Office Overhead?
Dental office overhead refers to the operating expenses practices incur to keep their doors open and treat patients. It encompasses staff salaries, clinical supplies, lab fees, facility costs, equipment, software, marketing, and administrative expenses, but not owner compensation.
Overhead is typically calculated as a percentage of collections. For example, a practice collecting $1 million and incurring $620,000 annually in operating expenses runs at 62% overhead [($620,000 / $1,000,000) x 100]. The remaining 38% goes toward owner compensation, debt service, and profit. Overhead determines net income, so managing it wisely directly impacts the bottom line.
Key Takeaways
- Overhead represents all the expenses that keep a dental practice running.
- The largest categories of overhead expenses are staffing, clinical costs, facility expenses, equipment, and patient acquisition.
- Overhead is typically expressed as a percentage of collections because it allows for more accurate period-over-period or comparative analysis.
- Fixed costs (such as staff salaries and rent) remain stable over time, but variable costs (including supplies and lab fees) rise and fall with patient volume.
- Calculating overhead regularly helps practices find areas to optimize costs without hurting the patient experience.
Dental Office Overhead Explained
Whether a practice sees 20 patients a week or 200, a substantial share of its revenue will likely go toward overhead. According to the American Dental Association (ADA), 41.5% of dentists cited overhead costs as one of the biggest challenges facing their practice, behind insurance issues (55.3%) and staffing (54.2%). Most practices break overhead costs into buckets earmarked for clinical operations, administrative work, marketing, and the dental facility itself.
Overhead is calculated as a percentage of collections because collections represent the actual cash received from patients and insurance payers. This is often a much lower number than production or billing, and it reflects what the practice earns once insurance adjustments and write-offs are cleared. A practice with heavy PPO participation, for example, might bill $1.2 million but collect only $900,000 after contractual write-offs. If the overhead incurred during that period was $500,000, the actual overhead percentage is 56% [($500,000 / $900,000) x 100], not 42% [($500,000 / $1,200,000) x 100]. Using collections grounds the calculation in economic reality, rather than arriving at an inflated figure that understates the true cost burden.
Fixed vs. Variable Overhead Costs
Dental accountants segment expenses according to their connection to patient volume. Fixed costs, such as rent, base staff wages, software subscriptions, insurance, and equipment leases, remain constant, even if patient volume fluctuates. Should patient volumes drop during a slow season, these costs often cause the overhead percentage to spike. For small and newer practices, fixed costs lead to high overhead percentages, as the same fixed cost base is parceled out across smaller revenues.
Variable costs, on the other hand, rise and fall with patient volume and case complexity—clinical supplies, laboratory fees, temporary staffing and overtime, and performance-based marketing. Tracking variable costs in relation to appointment schedules makes it easier to tell the difference between spending that reflects real productivity and spending that points to waste.
Dental Office Overhead Cost Breakdown
Controlling overhead starts with knowing where the money goes. Classifying expenses requires a detailed chart of accounts so accountants can allocate all transactions properly, which aids both expense monitoring and post-period analyses. The following eight categories are the most common overhead classifications for dental practices.
Staff Salaries and Benefits
Personnel costs, including wages, benefits, payroll taxes, and recruiting, typically represent the largest overhead category for dental practices. This covers clinical staff, such as hygienists and assistants, as well as administrative staff, such as front-desk and billing. When setting staff levels, practices should compare their patient volume and mix with staff productivity measures and reassess levels and performance expectations over time to match evolving demand. In a tight labor market, cross-training and continuing education can matter as much as salary when it comes to keeping good people.
Facilities
Facility-related expenses include rent or mortgage payments, utilities, maintenance, property taxes, and building insurance. Geography is responsible for much of the variance within this category—rent in downtown Manhattan isn’t comparable to rent in rural Kansas, for instance. Lease agreements usually run 5 to 10 years, so effective negotiations during lease renewals are a key way to reduce these largely fixed costs. Practices can also lower utility costs through energy-efficient upgrades, such as LED lighting and smart HVAC controls.
Supplies and Consumables
Dental offices providing quality care must regularly replenish their supply of gloves, masks, composites, bonding agents, impression materials, anesthetics, and disinfectants. When supply costs run higher than expected, practices should be on the lookout for product variations that have complicated inventory tracking, poor inventory management controls that led to overordering or stockouts, or subpar vendor negotiations. Standardizing purchases, consolidating to fewer suppliers, and rebidding on contracts annually can bring meaningful savings without compromising clinical quality.
Lab Fees
Laboratory fees are incurred for crowns, bridges, dentures, implant prosthetics, and orthodontic appliances. High lab costs may point to overused premium labs for routine cases, unnecessary outsourcing of work that could be milled in-house, or high remake rates. Practices with internal CAD/CAM technology for designing and fabricating these restorative items may enjoy lower lab fees but also incur higher costs for equipment, consumables, and staff time for operating the mill.
Dental Equipment
Dental equipment includes major assets like chairs, X-ray machines, sterilization units, air compressors, and imaging technology. Unlike supply purchases, equipment purchases above a certain threshold are capitalized on the balance sheet and expensed over time through depreciation, rather than recorded as immediate operating expenses. According to the ADA, equipment and supply costs rose 5% in the first nine months of 2025, making purchasing decisions more consequential. For major investments like CAD/CAM systems, ROI depends heavily on utilization—the more cases, the lower the per-unit cost.
Software Licenses
Day-to-day dental operations increasingly rely on practice management software, digital imaging systems, electronic health records, patient communication and scheduling platforms, and revenue cycle management tools. These specialized digital solutions must meet all relevant privacy standards, such as HIPAA in the United States and GDPR in the European Union. Over time, subscription creep can set in as practices continue to pay for overlapping or redundant systems; periodic audits can spot consolidation opportunities.
Patient Acquisition
Dental offices acquire new patients through digital advertising, search engine optimization, print marketing, direct mail, and referral programs. The key metric isn’t the percentage spent but the return on investment—specifically, whether the lifetime value of acquired patients justifies the acquisition cost. New or expanding practices typically spend more on patient acquisition than established practices that benefit from strong referrals.
Professional Expenses and Insurance
This category covers risk management and compliance expenses, such as malpractice insurance, general and umbrella liability coverage, property and equipment insurance, cyber and data breach insurance, OSHA compliance costs, and professional memberships. Premiums vary significantly by specialty, claims history, and location. For example, specialists offering higher-risk procedures may face higher premiums than general dentists.
Dental Practice Overhead Percentage Benchmarks
Benchmarks provide a starting point for evaluating how a dental practice stacks up. But no two practices are identical—their different priorities, staffing setups, patient bases, and specialties mean financial numbers only go so far.
Dental Practice Overhead Benchmarks
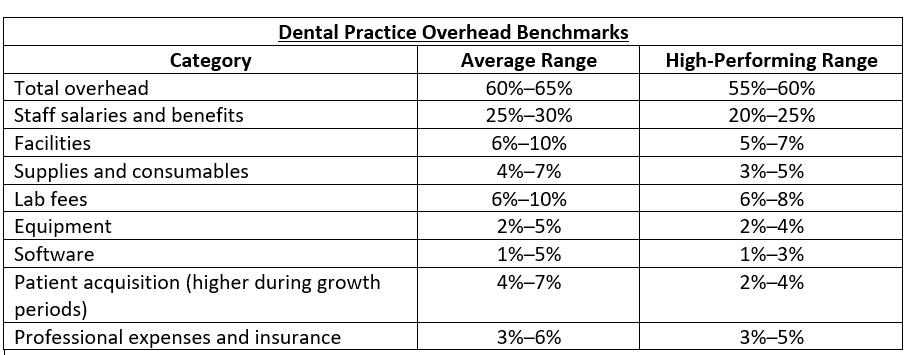
Tracking overhead over time is usually more meaningful than hitting a generally recommended number. Watch for upward trends and pay attention to how spending decisions affect the bigger picture. Several factors can push the ideal range in either direction:
- Practice size: Smaller practices often pay higher overheads because fixed costs must be covered by a smaller revenue base. Newer practices also pay more for patient acquisition and marketing until they’re established enough to rely on referrals and word of mouth. As practices grow, overhead percentage usually declines.
- Location: Urban practices in high-cost markets usually incur higher facility and labor costs than their suburban or rural counterparts. For example, a Los Angeles practice with 67% overhead may be operating with better spending discipline than a rural practice at 61%. Also, urban practices may be able to charge higher fees, ultimately bringing overhead percentages down.
- Specialty: Different specialties have different cost structures and obligations. Orthodontic practices, for example, tend to have lower supply and lab costs than general dentistry, while oral surgeons often carry higher facility and staffing requirements. These variances matter when comparing performance to industry benchmarks.
- Growth phase: Practices investing in expansion—be it a new location, better equipment, hiring blitzes, or increased marketing—may deal with temporarily higher overhead in order to earn future returns. Regular monitoring helps distinguish temporary spikes from sustained cost creep.
Calculating Dental Practice Overhead
Getting an accurate read on overhead takes solid data and some number-crunching. The following steps outline how dental CPAs calculate overhead percentage using data pulled directly from the profit and loss (P&L) statement:
1. Pull up your P&L statement: Use a full 12 months of financial data to smooth out seasonal fluctuations in patient volume and expenses. Accounting software can automatically generate P&L statements aligned with the practice’s preferred accounting rules. Many dental practices use cash-basis accounting, which recognizes revenue when cash is received, rather than accrual accounting, which records revenues and expenses when they’re earned or incurred.
2. Organize the expenses into categories: Assign each expense line item to a category, such as personnel, clinical supplies, lab fees, facility, general business/administrative, technology, marketing, insurance, or professional expenses. Bookkeepers should remove owner compensation, profit distributions, and personal expenses from overhead calculations.
3. Add the overhead expenses together: Total all operating expense categories. This sum represents the overhead in dollars, which can then be used for historical comparisons, trend analyses, and percentage calculations.
4. Divide expenses by total collections: Divide total operating expenses by gross collections (not what was billed) and multiply by 100. For example, $910,000 in expenses divided by $1,500,000 in collections multiplied by 100 equals 61% overhead. Separately calculating each category can help identify areas that may warrant additional scrutiny.
5. Identify your ideal dental practice overhead: Assess prior performance and any available industry reference points to set a realistic target for overhead spending. Adjust these targets according to practice size, specialty, and location before making one-to-one comparisons. The goal isn’t to match generic benchmarks but to establish expectations that will provide a foundation for financial strategies that can get spending back on track.
6. Develop a strategy to reduce overhead: If total overhead is exceeding targets, focus first on the largest categories to achieve the most meaningful improvements. A single category with high waste may be driving much of the total variance; thus, even minor adjustments can increase profitability. Set category-level targets and regularly monitor progress to spot stagnation or new issues early, rather than waiting for year-end reviews.
Tips for Optimizing Dental Practice Overhead
Controlling overhead doesn’t mean cutting corners on patient care or skipping investments in new technology. It means knowing where the money goes and making deliberate choices about expenditures. These six strategies help practices minimize waste, negotiate smarter, and use technology to keep costs in check:
1. Monitor expenses: Calculate overhead weekly or monthly rather than just at the financial close. Through regular expense monitoring, practices can stop runaway spending before more funds go toward unnecessary supplies or overstaffed shifts. Track each category against trailing 12-month trends and rolling forecasts to identify which expenses are drifting upward and how best to pivot on spending strategies.
2. Enact cost-control measures: Standardize your supply orders by identifying high-spend items and consolidating vendors on the basis of quality and cost-effectiveness. Automated inventory or procurement systems can set minimum stock levels and reorder points to prevent overordering and expired supplies.
3. Join a group purchasing organization (GPO): GPOs aggregate purchases across multiple practices to earn higher discounts with major suppliers. GPO membership can lead to significant savings on necessary supplies, giving independent practices the benefits of scale that were traditionally available only to larger groups.
4. Consider a different supplier or renegotiate your existing contracts: Annual rebidding or price-match requests prevent prices from creeping up unnoticed and create accountability for underperforming suppliers. When it comes to lab work, many practices assign tiered services by complexity, giving simpler restorations to volume-efficiency labs with lower per-unit costs and sending complex or aesthetic cases to premium partners.
5. Optimize scheduling and service KPIs: Routine services, such as cleanings and checkups, strengthen revenue and lead to strong patient relationships, but they require careful scheduling and labor allocation. Automated appointment reminders and digital patient portals help practices limit the number of no-shows and frequency of late cancellations. Inefficient check-in and checkout procedures can lead to unplanned overtime, escalating overhead and labor costs. Targeted metrics, such as no-show rates and chair utilization, help quantify inefficiencies and pinpoint where to focus improvement efforts.
6. Add automation and AI software: Automated billing, insurance verification, patient communications, and recall management can reduce overhead costs and administrative bottlenecks. Real-time dashboards give practices instant visibility into overhead costs as they accrue, while AI-powered tools flag issues early, such as accounts at risk of delinquency or billing anomalies.
Decrease Your Dental Office’s Overhead With NetSuite ERP
Keeping staff costs, supplies, lab fees, and facility expenses in check is hard when you can’t see what’s actually happening in your operations. NetSuite Dental ERP for Practice Management consolidates financial management, inventory tracking, and reporting on a cloud-based platform, automatically categorizing expenses as transactions occur. Customizable dashboards let practice managers sort costs by category, location, and provider, with built-in alerts that flag anomalies or cost variances before they compound into budget deficits. NetSuite’s built-in inventory features integrate with scheduling and procurement modules to automate reorders and maintain sufficient supply levels at optimal prices, even as patient volume fluctuates.
NetSuite’s Inventory Dashboard
Overhead is what separates the revenue a dental practice collects from the profit it keeps. By tracking overhead over time, categorizing each expense, and addressing costs as they fall out of line, practice owners can find places to cut costs and increase profits. Specific targets vary by practice, but what matters stays constant: controlling costs, watching the trends, and adjusting spending without compromising patient care.
Dental Practice Overhead FAQs
What is the average overhead of a dental office?
Average dental practice overhead usually falls within 60% to 65% of total collections, but it can vary significantly by practice size, location, and specialty.
How do you reduce overhead in a dental office?
First, calculate your monthly overhead and identify which categories rise above expectations. From there, develop targeted strategies to address specific pain points, such as joining a group purchasing organization to get discounts on supplies or integrating scheduling and labor systems to minimize patient no-shows and overtime costs. Prioritize the categories with the largest overhead percentages to maximize impact.
What’s the largest overhead investment for a dental practice?
For most practices, labor makes up the largest overhead category. This includes wages for hygienists, dental assistants, front-desk staff, and billing personnel, as well as health insurance, retirement programs, payroll taxes, and recruiting costs.
Why does overhead cost control matter to a dental practice?
Overhead determines how much revenue remains after paying the office’s expenses. Every dollar spent on overhead directly subtracts from profits and affects the practice’s ability to compensate owners and cover debt obligations. Keeping overhead under control is how practices stay financially healthy, finance growth, and survive slow periods.







